
Running with Plantar Fasciitis
Plantar fasciitis is an epidemic amongst our society and has resulted in numerous treatment plans that vary from one health care provider to another. Guidelines for treatment protocols exist and even those differ from one specialty to another. Plantar fasciitis is searched monthly on google over 550,000 times with web pages revealing information ranging from explaining the cause to sites marketing gimmick treatment devices to take advantage of those suffering in pain.
The purpose of this post is to give hope to those suffering and hopefully point runners in the right direction who are trying to overcome this chronic condition.
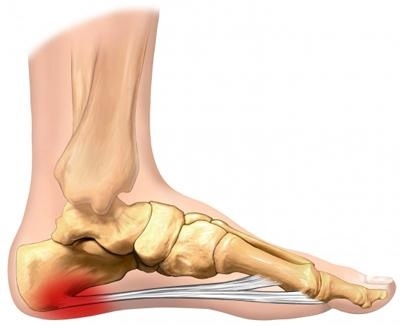
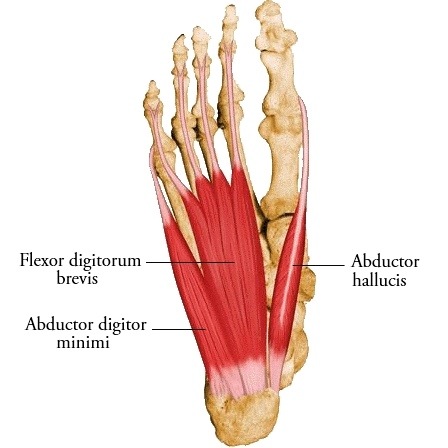
To begin, plantar fasciitis has been described as an inflammation of the plantar fascia – a band of tissue that originates on the heel bone and fans out to the toes of the feet providing structure and protection to the underlying vessels, nerves, and muscles of the foot. Surprisingly, studies have demonstrated inflammatory cells are not present within the plantar fascia in those suffering from the condition suggesting it may not be “inflammation” within the plantar fascia. There are 3 muscles that attach to the heel bone in conjunction with the plantar fascia – the abductor hallucis, abductor digiti minimi, and flexor hallucis brevis. These muscles develop tendonitis when overused or weak from being in shoegear all day. This leads to pain upon arising in the morning, and again throughout the day after increased activity.
The muscular tissues that are inflamed are attempting to heal themselves and need to be stretched or warmed up to reduce the pain. Then, after periods of activity, the muscles again become sore leading to pain later in the day. The result – chronic pain to the heel and or arch area.
When runners develop plantar fasciitis, what should they do?
In my practice, if they are able to complete a run without pain, I encourage the patient to continue running. I then advise:
1. anti-inflammatories if they are able to take them
2. Stretching exercise to be performed 4 times a day
3. Ice 30 minutes as many times a day to the area
4. Barefoot activities 20-30 minutes per day to encourage foot strengthening gradually increasing weekly
5. Flat shoes without a heel to promote anatomic positioning of the foot and rest of body
6. Splinting may be done but only temporarily
If the condition persists, cortisone injections are utilized to aid in decreasing the inflammation. They are safer in theory then NSAIDS as they are local and not systemically absorbed.
If the above treatment fails, then the condition is most likely secondary to the runner’s form which will need to be analyzed and changed. I simply tell patients who have tried all of this and failed, then something they are doing at home, work, or while running is precipitating the condition.
Orthotics are not the answer for my patients who are runners as they simply promote weakening of foot musculature.
What about a plantar fasciotmy? (Surgical release of the plantar fascia)
To reiterate, studies show that after performing a plantar fasciectomy (surgical release of the plantar fascia) the tissue sent to the pathologist revealed no inflammatory changes. This leads many practitioners to believe the condition is more muscular which explains the pain upon rising in the morning or after periods of rest. Why then would cutting the plantar fascia be indicated to help overcome this condition? As a surgeon, I stopped doing this procedure several years ago as the studies do not advocate it’s relevance.
Consider this, why would we cut an anatomic structure that process structural integrity to the foot, protects the underlying vessels, and is not even scientifically proven to be inflamed in clinical studies?
Therefore, treat this like a tendonitis.

Share with the running community!

Related Posts



About The Author
Dr. Nick Campitelli
Dr. Campitelli is a podiatrist in Akron, OH specializing in foot and ankle surgery with an interest and enthusiasm for running as well as helping runners with injuries. For the past several years he has been treating running injuries in patients by fixing their form and transitioning them to minimalist shoes. Having treated runners with all types of injuries through conservative measures with orthotics and shoe gear changes to reconstructive foot and ankle surgery, Dr. Campitelli has brought what works best and is most current to his practice as well as the Akron and Cleveland running communities.
I have been suffering with Plantar Fasciitis or fat pad syndrome for about 6 months now. I am finally able to run again but still experience some soreness/ tenderness in my heel. I feel that my calves are one of the primary issues and am constantly have to massage them or roll them out to prevent knots. Also trying to run with relaxed calves helps (this is hard!) During my rehabilitation, I could not walk barefoot without pain so chaco sandals really helped. Now that I am running I am wearing Altra provisoness which is a zero drop but supportive shoe. I will gradually progress back to a more minimalist shoe. I am also a farmer during the Spring, Summer and Fall. Do you feel like wearing a zero drop work boot ( I use a wedge work boot and shave the wedge to zero drop) during my work hours (10+ per day) is adequate support for my feet after long runs? Thanks in advance! Rebecca
Thanks for another informative post! Recently I’ve come across a lot of evidence that anti-inflammatories can often impair recovery or even exacerbate inflammation, and that inflammation can be a critical component of healing. I’m curious about your thoughts on this issue, considering your advice to take anti-inflammatories and ice? Although this is only anecdotal, I’ve personally only had negative experiences with anti-inflammatories and avoid them entirely.
Thanks for another informative post! Recently I’ve come across a lot of evidence that anti-inflammatories can often impair recovery or even exacerbate inflammation, and that inflammation can be a critical component of healing. I’m curious about your thoughts on this issue, considering your advice to take anti-inflammatories and ice? Although this is only anecdotal, I’ve personally only had negative experiences with anti-inflammatories and avoid them entirely.
Loved and agreed with a lot of this article.
Not a fan of anti-inflammatories. Weakens those structures. Disagree you treat it as a tendinitis. Treat as tendinosis.
Also think orthotics way over prescribed. Might be a part of the solution though if its a foot structure issue (rare).
Heartily agree on strengthening and barefoot work. Fasciotomy will be looked at like leeches in the not too distant future.
See this every day. Treat the symptoms (manual work, night splint, etc) and work on the root causes.
Root cause can be tricky because in our experience, PF is secondary to another mechanical issue.
do you think a 4mm drop on the nb minimus shoes would be ok for plantar fasciitis?
Yes. That’s a great shoe. If you are used to the drop and have adapted its fine. Ultimately I prefer a flat shoe bit four is mild
do you think a 4mm drop on the nb minimus shoes would be ok for plantar fasciitis?
Yes. That’s a great shoe. If you are used to the drop and have adapted its fine. Ultimately I prefer a flat shoe bit four is mild
Hi Dr. Nick
I’ve read your article and I liked it very much. Although, it was very strange to me that you don’t recommend orthotics for plantar fasciitis becouse that’s the only treatment I give and it does a very good work. of course not all the time, but for many athletes it improves the inflamation.
I’ll be happy if you can visit my site to understand the benefits of my Orthotics.
Best wishes,
Tamir
Hi Dr. Nick
I’ve read your article and I liked it very much. Although, it was very strange to me that you don’t recommend orthotics for plantar fasciitis becouse that’s the only treatment I give and it does a very good work. of course not all the time, but for many athletes it improves the inflamation.
I’ll be happy if you can visit my site to understand the benefits of my Orthotics.
Best wishes,
Tamir
I had PF for a year when I started running 3 years ago. Since then I have adjusted my form + changed to 4mm drop shoes. I have been feeling twinges in my heel when I get up for the past week. I run in Kinvara 3s and wear only flat shoes at this point in regular life. My summer flats are a barefoot type shoe and I am wondering if the PF is flaring because now I am wearing harder soled boots + shoes (it is winter in northern michigan!) I really haven’t changed anything else and have reduced mileage in the last month. Also, I do have a pair of Altra Intuitions. They feel sloppy when I run in them but I do like them for walking. Should I try running one day a week in those for a change as well? Thanks for your input.
I would advise trying to avoid the hard soled boots before I would switch my running shoes. Sounds like ur running shoes are working. As long as your form is good the shoes you have sound fine. Stretch more and ice and get rid of boots!!
I had PF for a year when I started running 3 years ago. Since then I have adjusted my form + changed to 4mm drop shoes. I have been feeling twinges in my heel when I get up for the past week. I run in Kinvara 3s and wear only flat shoes at this point in regular life. My summer flats are a barefoot type shoe and I am wondering if the PF is flaring because now I am wearing harder soled boots + shoes (it is winter in northern michigan!) I really haven’t changed anything else and have reduced mileage in the last month. Also, I do have a pair of Altra Intuitions. They feel sloppy when I run in them but I do like them for walking. Should I try running one day a week in those for a change as well? Thanks for your input.
I would advise trying to avoid the hard soled boots before I would switch my running shoes. Sounds like ur running shoes are working. As long as your form is good the shoes you have sound fine. Stretch more and ice and get rid of boots!!
I have been trying to run with plantar fasciitis since 2006. But I have never had pain in my heel, it has always been high up in the middle of my foot and the only pain I have is after I have run about a mile and occasionally when I play basketball long and hard. I have never been able to find any thing on PF for those who don’t have it in the heal, but in the upper middle of the arch, the flexor digitorum brevis. What are some recommended shoes and treatment for my specific case of PF? Specially fitted orthodics don’t work and I have a pair of zero drop minimalist shoes that i have been wearing daily and running in but I still have the same result with those as I have with asics and saucony which I ran track and cross country in when my PF first developed. Whats your take on this? Thanks!
I have been trying to run with plantar fasciitis since 2006. But I have never had pain in my heel, it has always been high up in the middle of my foot and the only pain I have is after I have run about a mile and occasionally when I play basketball long and hard. I have never been able to find any thing on PF for those who don’t have it in the heal, but in the upper middle of the arch, the flexor digitorum brevis. What are some recommended shoes and treatment for my specific case of PF? Specially fitted orthodics don’t work and I have a pair of zero drop minimalist shoes that i have been wearing daily and running in but I still have the same result with those as I have with asics and saucony which I ran track and cross country in when my PF first developed. Whats your take on this? Thanks!
This was very informative information on plantar fasciitis. I suffered from PF three years ago and it took me a long while of lots of trial and error before I found a cure for my PF. Stretces work best for me but in your article i notice you mentioned barefoot walking. While i ad plantar fasciitis it seem very unconfontable walking barefoot with my fascia in pain. In my opion i would not recommend barefoot walking as i tink it would just help tear the fascia. I have more information on this subject on my blog intitled How to cure Plantar Fasciitis